
Lego construction for operating rooms
Modular operating rooms are being seen more and more on the market. It takes less time to get it up and running compared to a traditionally built hospital. It´s cost-effective, time-saving, and can be taken down and moved when it´s not needed anymore. However, it can negatively affect acoustics due to the low sound absorption of the modular material. Especially since there is no tradition to use sound-absorbing material but use the same hard-surfaced material for both walls and ceiling.
Last year a new modular constructed operation department was built and we had an opportunity to have it measured acoustically. We have previously published measurements on great acoustics in modular operating rooms in a construction docked onto a house a few stories up. But this time it was a full building attached to an operation department on the ground floor. The building material of the walls was different this time and it is relevant to find out if the acoustics would be different.
Why do acoustics need our attention?
Over the last 40 years, hospitals’ noise levels have steadily increased [1]. Operating rooms can be particularly noisy and sound peaks can reach 110dB when drills and saws are in use. Sound levels at that level can damage your hearing and are perceived as very loud. Poor acoustic environment and high sound levels may affect the ability of the staff to receive proper oral instruction. It also affects their perceived stress levels and well-being [2, 3].
What can be done to reduce this noise? It requires a combination of actions; alteration of human behavior, default settings and lower functional sounds on med-tech devices, and the use of sound-absorbing materials to deal with excess sound energy and unwanted reflections [4].
Sound-absorbing material can improve the sound environment, as shown in several studies. The effect has an impact on the staff´s work environment, well-being, stress, and the patient´s experience of receiving care [5,6].
Project
The Northern Älvsborg County Hospital (NÄL) in Sweden is an emergency hospital that conducts almost 9000 planned and emergency operations every year. On the existing premises, which have been in use for about 30 years, there have been repeated roof leaks in recent years, which eventually became an acute problem.
This meant that one of the operating departments was closed rather quickly. Since a renovation process takes several years, a quick alternative was needed to keep operations up and running. The solution involved temporary replacement facilities in the form of module operating rooms.
Working quickly, Q-bital Healthcare Solutions with their Swedish distributor, Meditek, delivered 4 fully equipped modular operating rooms in just six months to NÄL.

The modules consist of four operating rooms (50m2) with corresponding preparation rooms, a material storage room that is 50m2, a sterile storage room of 25m2, disinfection rooms, and a long corridor from the existing building to the operations modules.
Choosing the right material
The modular wall consists of a high-pressure laminate (HPL). But since the acoustics was given proper attention the ceiling was changed from HPL to a sound-absorbing ceiling with glass mineral wool, with absorption class A. Operating rooms can have many different material demands such as the surface having to withstand regular cleaning and disinfection, maximum levels of air permeability, and so on – they vary in different countries.
Ecophon Hygiene Performance™ was chosen as it can be disinfected and is classified ISO 4 according to ISO 14644-1
The operating rooms were to be used for gynecological and general surgery with a maximum value of <10 CFU (colony forming units) throughout the room. A CFU is a unit commonly used to estimate the concentration of microorganisms in a test sample. Most operating rooms have a set minimum value often for different places in the room, in this case <10 CFU at any given spot. For this Swedish project, Ecophon Hygiene Performance™ was chosen as it can be disinfected and is classified ISO 4 according to ISO 14644-1. It also complies with the CFU target [7].
Acoustic measurements
T20
So what did the measurements show? The required reverberation time (T20) is ≤0.6 seconds (250-4000Hz) and ≤0.8 seconds at 125Hz according to Swedish Standard 25268 building regulations for hospitals [8]. Many countries do unfortunately not have a recommendation for operating rooms. But for example in Denmark, we will find T20 to be <0.6 seconds as well, and in Germany 0.7-0.8 seconds.
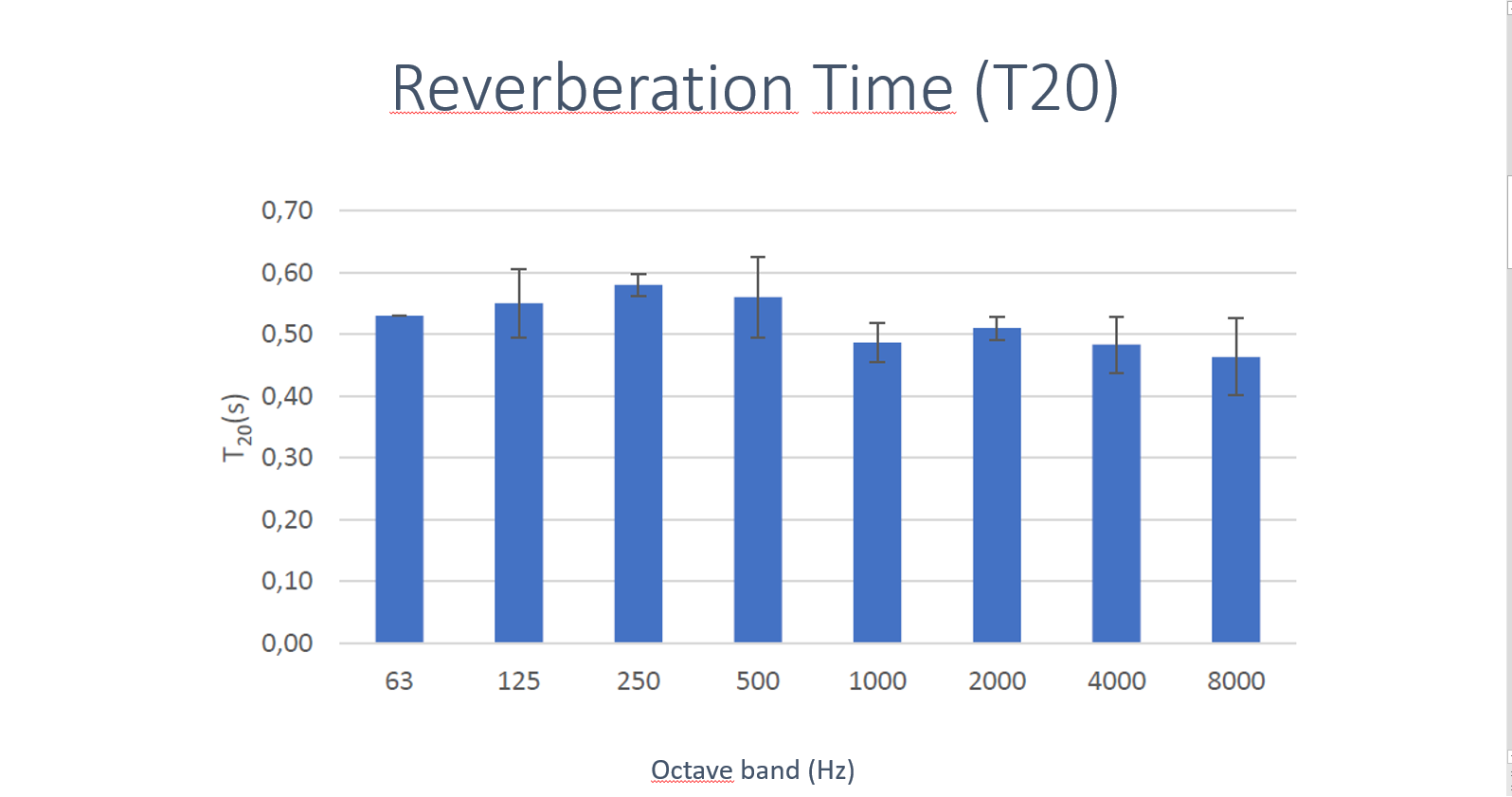
Reverberation time shows a mean of 0.5 seconds and 0.6 seconds at 125Hz. Very good results and the building regulations are met and we did specifically well at 125Hz!
The reverberation time is mainly influenced by the surface treatment of the room. A high reverberation time can make a room sound sonorous, while a short reverberation time subdues sounds in the room.
We are confident that this modular operating room has the very best conditions of reverberation time possible!
C50
We also chose to measure Speech Clarity (C50) to better understand the working environment, even though it is not included in the standard.
As previously mentioned the sound environment can be challenging with high sound pressure levels.
There is also a challenge in receiving speech due to a few factors in this room type. Staff will have their ears and mouth covered which muffles the speech and possibly affects the ability to determine the direction of the sound source. They are also placed in different zones in the room. The surgeon(s) and operating nurse will have their backs on the other staff. Other staff in the outer zones are not allowed to move closer to better hear what the surgeons say. If possible, working to improve speech clarity is beneficial for these challenging work environments.
Speech clarity concerns the quality of speech transfer to the listeners. The sound that reaches the listener first is called direct sound. This is followed by early reflections. The early reflections that reach the listener within 50msec are integrated with the direct sound and thus positively affect speech clarity. The reflections that come later may be perceived as disturbing. C50 measurement compares the sound energy in early sound reflexes with those that arrive later.

C50 was also shown to be good in the results above. The aim for good speech intelligibility is generally considered 6dB or higher. In this case, the mean between 63-8000Hz was calculated as 7.9dB.
Above all, a high C50 is strongly related to good speech intelligibility. Meaning our brain simultaneously integrates the early reflections and the direct sound, which makes us perceive the sound more stronger and with better clarity.
C50 is primarily influenced by the design and layout of the room. It is also strongly affected by the proportion of reflective surfaces that are in direct proximity to the sound source.
The amount of diffusing material, such as pendants and machinery, also influences speech intelligibility.
Background noise
The background noise was measured at 41.1dB LAeq and 55.2dB LCeq. And the primary sound source was the advanced ventilation system (TcAF ‘Opragon’ by Avidicare).
When measuring the Speech Transmission Index (STI) at a distance of 2.9 meters, we calculated an STI of 0.53. STI is a measure of how well speech information is transmitted from speaker to listener. It gives a numerical value between 0 and 1. An index of 1 means that a speech has perfect intelligibility. Unlike C50, STI takes into account background noise in the room and the distance between the speaker and listener. The relatively low value is probably due to the background noise. It would be considered fair for a native speaker but could be problematic for a non-native listener [9]. Therefore it could be advised to increase the STI in the future. For instance by lowering the background sounds and adding absorption and diffusions to the walls.
G
Sound Strength (G) is a measure of the room’s ability to absorb sound energy and how noisy a given sound source will be experienced. It is affected by the size of the room and the amount of absorbent material.
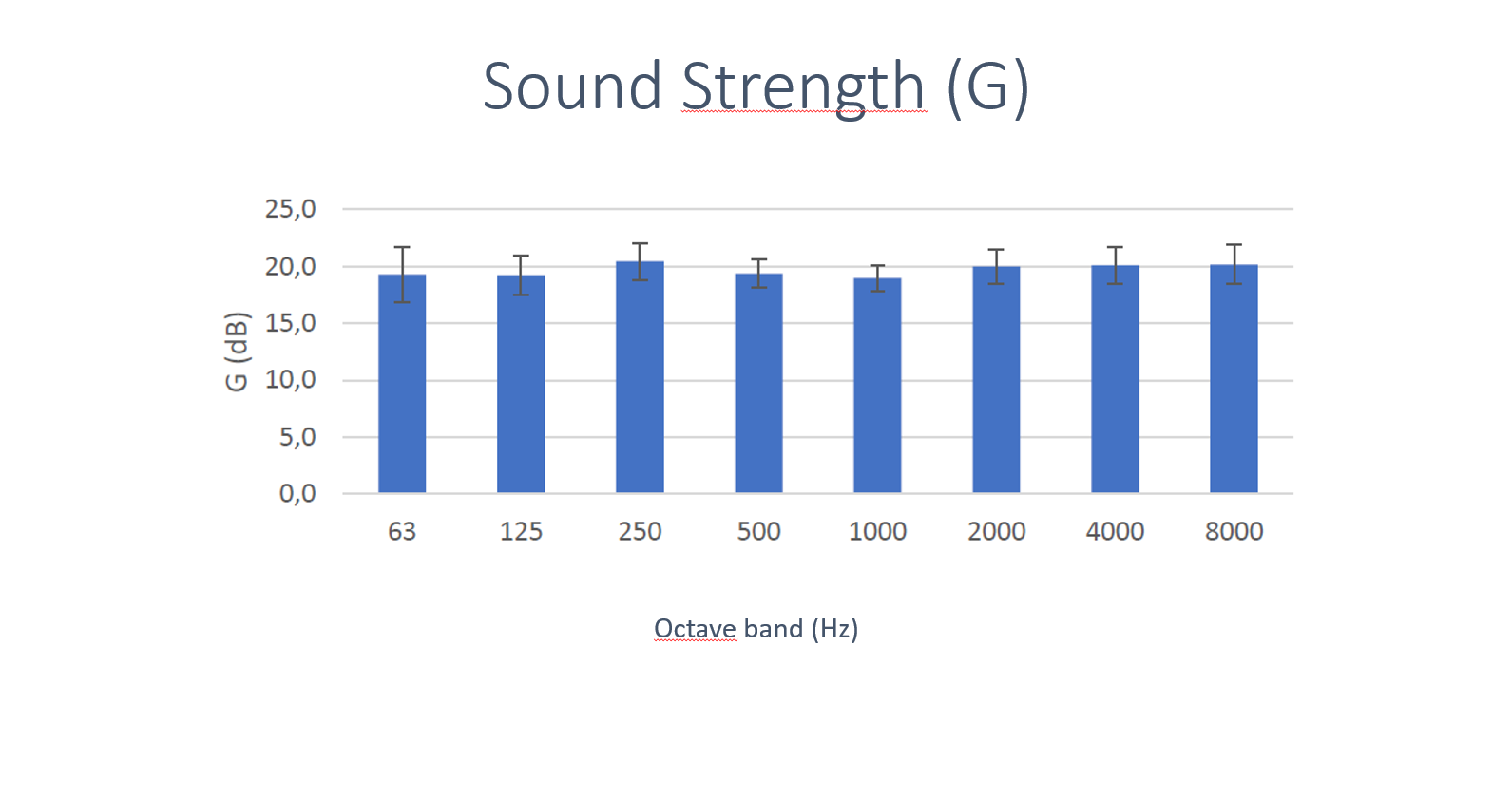
Strength states the sound level in the room in relation to the sound level in an anechoic room with the same sound source. Values below 20dB are generally considered good, but we don´t have much literature and studies on the application in hospital facilities.
When building with other wall materials than the usual, it is of value to measure what kind of impact it has on G. In these modular operating rooms we measured a mean of 19.7dB.
Considering the high sound peaks that can be experienced it is positive with a low G value to not increase the peaks louder than necessary.
Good outcome
Great care has been put into creating the best possible acoustics to fulfill the requirements and address speech intelligibility and acoustic comfort.
Feedback from staff is very positive and we can conclude that high specialists’, areas such as an operating room, can be built with a modular technique and have a supporting sound environment if the acoustic outcome is well catered for. As we can see an increase in these building techniques we need to have a clear picture of how their choice of material will influence the work environment and fulfillment of acoustic regulations, using more acoustic parameters than only reverberation time seems like a responsible way to go.
Sources
[1]. IJ. Busch-Vishniac, JE. West, C. Barnhill, T. Hunter, D. Orellana, R. Chivukula: Noise levels in Johns Hopkins Hospital. J Acoust Soc Am. 2005;118:3629–3645.
[2]. Sentinel Event Alert Issue 50: “Medical device alarm safety in hospitals” A complimentary publication of Issue 50.The Joint Commission, 2013.
[3]. EE. Ryherd, S. Okcu, J. Ackerman, C. Zimring, K. Persson Waye: “Noise pollution in hospitals: Impacts on staff”, J. Clin. Out. Mgmt. 2012, vol 19, no 11, p491-500
[4]. Engelmann CR, Neis JP, Kirschbaum C, Grote G, Ure BM. A noise reduction program in a pediatric operation theatre is associated with surgeon’s benefits and a reduced rate of complications: a prospective controlled clinical trial. Ann Surg. 2014;259:1025–1033.
[5]. MacLeod M, Dunn J, Busch-Vishniac IJ, West JE, Reedy A. Quieting Weinberg 5C: a case study in hospital noise control. J Acoust Soc Am. 2007;121:3501–3508.
[6]. Blomkvist V, Eriksen CA, Theorell T, Ulrich R, Rasmanis G. Acoustics and psychosocial environment in intensive coronary care. Occup Environ Med. 2005;62:e1.
[7]. ISO 14644-1:2015. Cleanrooms and associated controlled environments – Part 1: Classification of air cleanliness by particle concentration.
[8]. Swedish Standard Institute. SS 25268:2007 Acoustics – Sound classification of spaces in buildings –Institutional premises, rooms for education, preschools, and leisure-time centers, rooms for office work and hotels
[9]. SS-EN 60268-16:2020. Ljudanläggningar – Del 16: Objektiv bedömning av taluppfattbarhet med hjälp av talöverföringsindex.