
Thea Mathilde Larsen, Research Assistant at DTU (Technical University of Denmark), has recently defended her master thesis project ‘Study of Room Acoustics and Noise at Bispebjerg and Frederiksberg Hospital’, on two Danish projects. A study aimed to investigate the need for improving room acoustics in hospitals along with investigating staff’s opinion of the noise problem.
It is no secret that the process itself (doing acoustic research in a hospital) is a huge amount of work. Just getting into different wards with the acoustic equipment – at night – in the morning – all day – is a challenge. Hygiene demands have to be controlled, including respect for nurses’ ‘peak hours’, respect for the patients, opening hours, arranging meetings with doctors, administration, cleaning personnel, etc. All of that alone is a master thesis!
Danish project – the two buildings
The two hospitals were built in 1913 (Bispebjerg) and 1903 (Frederiksberg) and they are both situated in Copenhagen and have together 3000 employees. Thea Mathilde Larsen writes in her thesis that:
‘… it was not until recently in 2013 that the Danish Building Regulation added guidelines to acoustics in hospitals..’
and that the guidelines state:
‘…the reverberation time in patients’ rooms should not exceed 0.8 s for the frequency bands 125-4000 Hz and the reverberation time in examination rooms and treatment rooms should not exceed 0.6 s for the frequency bands 125-4000 Hz, with a liberation of 20 % for 125 Hz.’
So what does it sound like in the hospitals today? Can the old buildings meet the demands of today? And what does the staff say about it? The short answer is – no the rooms are not fulfilling the demands and the staff complains.
Massive amount of data!
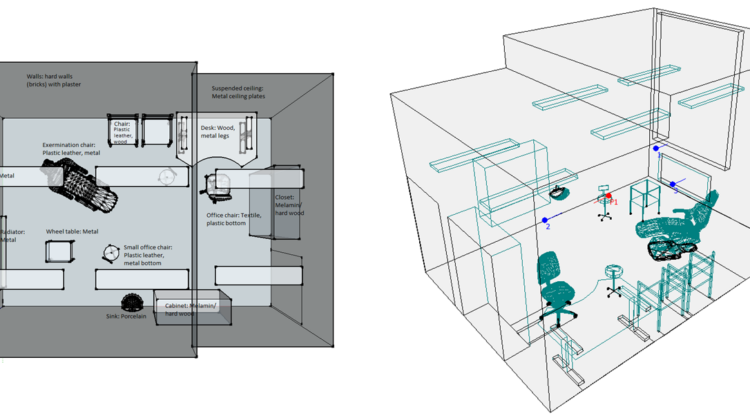
The project has a massive amount of data from room acoustic measurements in more than 20 different rooms- But one room, in particular, had our attention during the process – and it was also representing the typical challenges at Bispebjerg hospital (the listed building).
 We were interested in doing an intervention study in this room at the Dermatological department because the sound environment in the examination rooms, according to the staff was a catastrophe. We were told that the doctors had to use microphones to be heard by the patients (!) – even though the rooms were just ‘ordinary’ single examination rooms. In this particular department, a lot of the patients are elderly people. And knowing that ‘natural’ hearing impairment increases over time the room acoustics of these rooms are of great importance.
We were interested in doing an intervention study in this room at the Dermatological department because the sound environment in the examination rooms, according to the staff was a catastrophe. We were told that the doctors had to use microphones to be heard by the patients (!) – even though the rooms were just ‘ordinary’ single examination rooms. In this particular department, a lot of the patients are elderly people. And knowing that ‘natural’ hearing impairment increases over time the room acoustics of these rooms are of great importance.
Unfortunately, it was impossible to do the intervention (because of time), but measurements and simulations were done. Even though the building regulation only states values on reverberation time, Thea Mathilde Larsen chose to include other acoustic descriptors in her measurements and simulations to get a more detailed overview.
Measurements
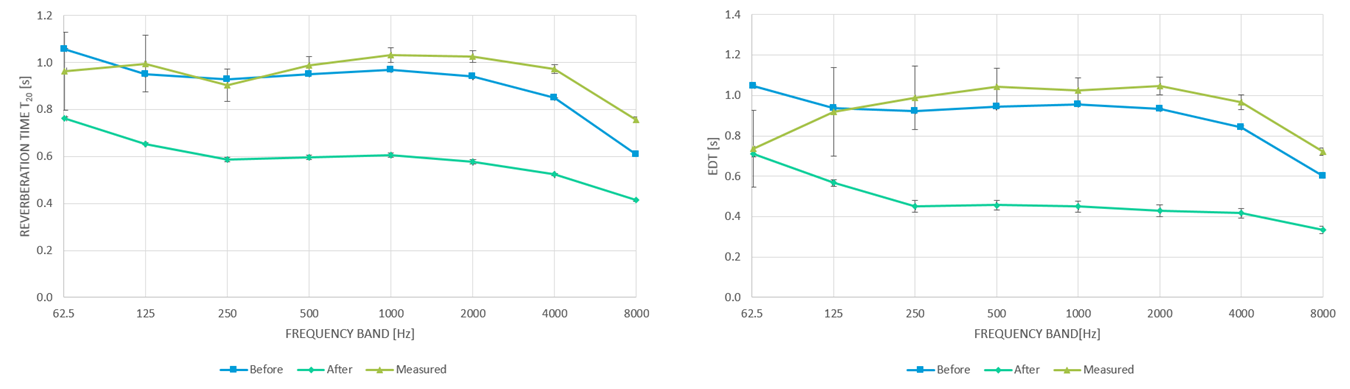
The measurements on reverberation time showed that T20 was over a second (!) in almost every frequency band. And EDT (which normally is said to have a stronger link to the actual human perception of sound) is just bad.

NB. Room D.Ex.12
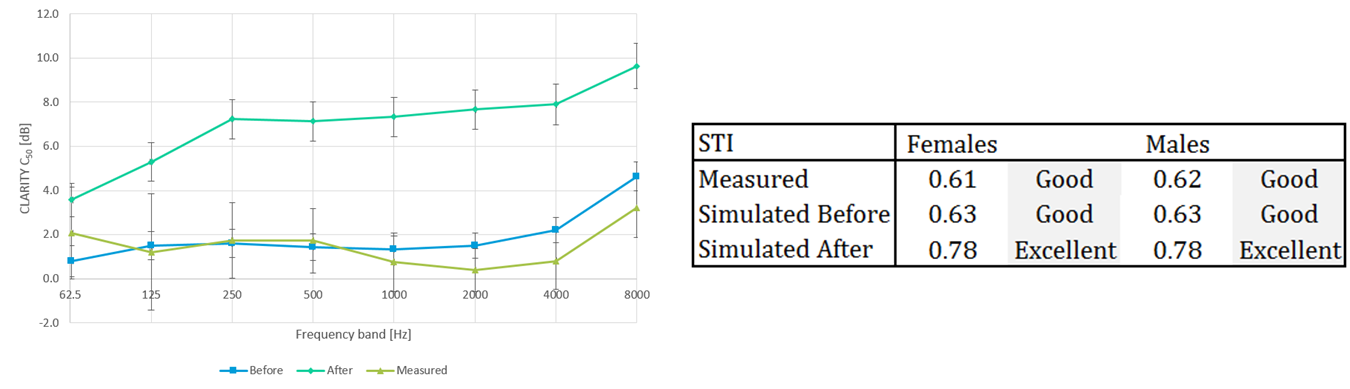
If we look into speech clarity descriptors it is more unclear to conclude a trend when comparing C50 and STI. The STI values are objectively ‘good’ – just above 0.6. But what the STI standard does not take into consideration here is what ‘good’ really is when you are older and maybe hearing impaired.
The standard presupposes normal hearing, no hearing loss, and no cognitive challenges. So in this case, ‘good’ could be bad in reality. When looking at C50 which is a more objective parameter we see values below 2 dB which must be objectively considered as room acoustic conditions not appropriate for clear communication. Knowing how doctors sometimes use microphones in this sound environment – I doubt that the patient experience gets any better.

NB. Room D.Ex12
Simulations instead of acoustic intervention
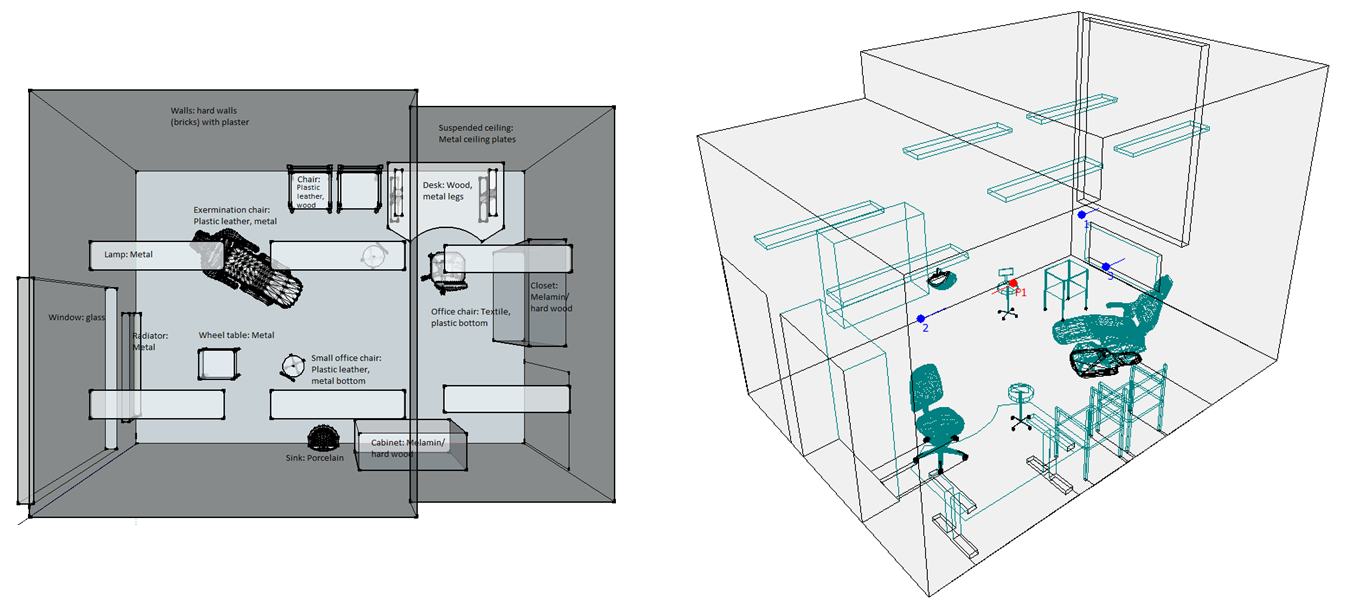
As mentioned the project should have included an acoustic intervention in this particular room – but because of lack of time, it wasn’t possible. It is extremely important to include hygiene staff in acoustic refurbishments. This is to secure that the acoustic product can reach the strong hygiene demands that can differ from department to department – from room to room. In this particular case, we had a meeting with the cleaning responsible and we found a solution that could have been used if we had the time.
The company Niras (consultant engineers company) made an Odeon simulation of the examination room. The results of this were quite clear: It is possible to meet the acoustic and hygienic demands with a suspended acoustic ceiling – and to reach satisfying values on speech clarity as well as respecting the legacy of this listed hospital building!
As the simulation values show – we have no problems with reverberation time. In this particular room, the EDT and clarity descriptors show a sound environment also suitable for communication with hearing-impaired people.
Danish Sound Innovation Network funding
The master thesis on Danish project has been defended already. However, it will continue in the following months with funding from the Danish Sound Innovation Network and with cooperation from Ecophon, Niras, Henning Larsen Arkitekter, and Hvidovre hospital.
The work to come will most likely look into a comparison with a ‘younger’ hospital (Hvidovre Hospital) and newly renovated departments. All to gain a clearer view of what ‘normal’ is regarding room acoustics in Copenhagen/Danish hospitals.
 NB. All figures and numbers used in this post are taken from the report ‘Study of Room Acoustics and Noise at Bispebjerg and Frederiksberg Hospital’ by Thea Mathilde Larsen, Research Assistant at DTU
NB. All figures and numbers used in this post are taken from the report ‘Study of Room Acoustics and Noise at Bispebjerg and Frederiksberg Hospital’ by Thea Mathilde Larsen, Research Assistant at DTU
Previous posts on the research project, including staff feedback, are available here.